

Categories
By: H.E. Mrs Toyin Ojora Saraki & John Oldfield
There is an invisibly simple way to assess whether a health system is structurally capable of delivering safe care, particularly at the moment when life is most vulnerable, and it is not found in policy declarations, national strategies, or investment pledges, but in the physical and operational conditions of care itself. Can a midwife reliably wash her hands between deliveries? Is clean water available at the point of care? Are sanitation and hygiene services sufficiently dependable that infection prevention is routine rather than improvised?
For over two decades, the Wellbeing Foundation Africa has worked at the intersection of maternal, newborn and child health, primary health systems, and community wellbeing, grounded in a simple but often overlooked truth: the quality of care a health system delivers is inseparable from the conditions in which that care takes place. Nowhere is this more evident than in water, sanitation and hygiene (WASH) in healthcare facilities, where the presence or absence of clean water, functional sanitation, and effective hand hygiene determines whether clinical care protects life or exposes it to avoidable risk.
This reality is most clearly understood not through abstraction, but through practice. Some years ago, a frontline midwife explained, without complaint or embellishment, why she preferred elbow-length gloves during deliveries. It was not just a matter of protocol or training; it was a practical response to uncertainty. When clean running water and soap could not be reliably guaranteed between patients, she adapted to reduce exposure. That explanation reflected what health workers and women had long understood: care continues even when systems fall short, but risk is redistributed onto those least able to bear it.
When a woman in labour enters such a facility, she may never know whether water will be available that day or whether hygiene between deliveries is assured. She places her trust in the system nonetheless. That trust is essential to care, and it is fragile. Where WASH is absent or unreliable, the burden of that fragility falls disproportionately on mothers, newborns, and frontline healthcare workers.
It was precisely this gap between lived experience and formal measurement that the global health community began to address more systematically during the United Nations Sustainable Development Goal era. The Millennium Development Goals delivered substantial progress in expanding household access to water and sanitation worldwide. At the same time, their indicators focused primarily on household coverage, which meant that conditions inside clinics, maternity wards, and delivery rooms were not consistently measured at the global level.
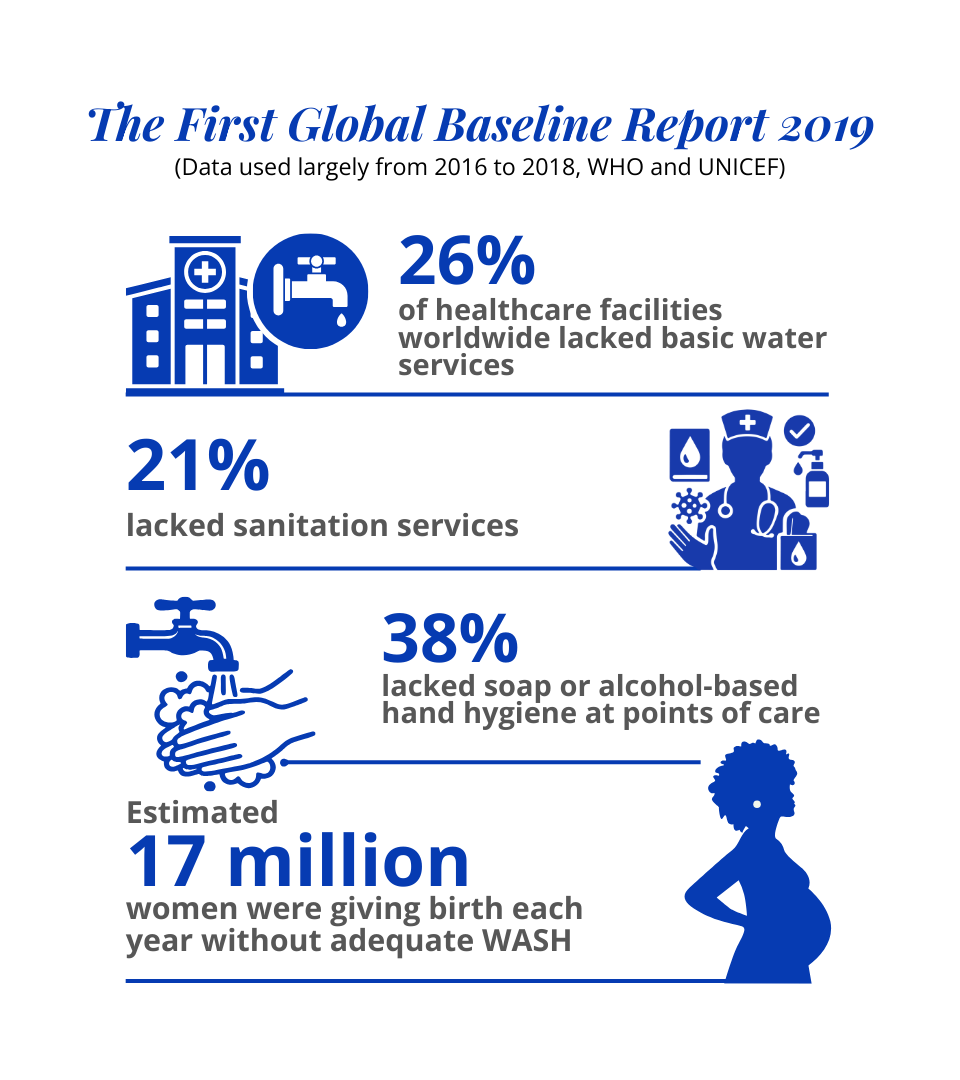
From 2016 onward, the WHO and UNICEF Joint Monitoring Programme introduced harmonised service ladders for water, sanitation and hygiene in healthcare facilities. The first global baseline report, published in 2019 using data largely from 2016 to 2018, showed that 26 per cent of healthcare facilities worldwide lacked basic water services, 21 per cent lacked sanitation services, and 38 per cent lacked soap or alcohol-based hand hygiene at points of care. In maternity care alone, an estimated 17 million women were giving birth each year in facilities without adequate WASH services during this period.
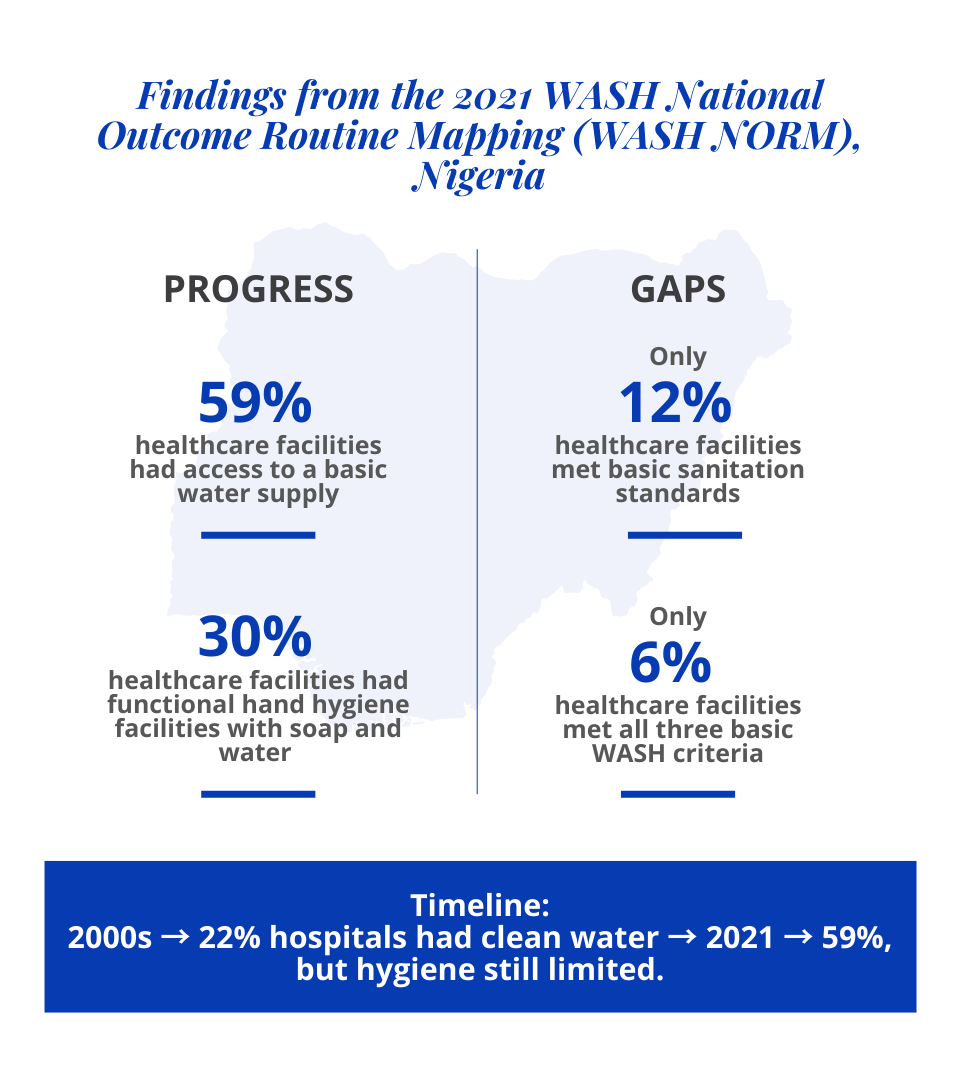
Nigeria’s experience aligns with this global evidence. Facility-level assessments conducted during the late 2000s and throughout the 2010s found that only about 22 per cent of Nigerian hospitals had reliable access to clean water at the time of assessment, with even lower availability of water and soap within delivery rooms. These findings were derived from structured facility surveys using internationally recognised methodologies and were understood as baseline diagnostics rather than permanent descriptors.
This evidence also sits within a longer arc of global political commitment to water and sanitation as human rights. In 2010, the United Nations General Assembly adopted Resolution A/RES/64/292, formally recognising access to safe and clean drinking water and sanitation as a human right essential to the full enjoyment of life and all human rights. This commitment was further clarified in 2015 through UN General Assembly Resolution A/RES/70/169, which affirmed the distinct human rights to water and to sanitation and specified that services must be sufficient, safe, acceptable, physically accessible, affordable, and delivered in ways that ensure dignity and privacy. While not legally binding, these resolutions established a rights-based normative framework that continues to guide national policies, global standards, and development programming across community and health system settings.
More recent national data reflect both progress and persistent gaps. The Nigeria WASH National Outcome Routine Mapping survey, conducted in 2021, reported that while 59 per cent of healthcare facilities had access to a basic water supply service, only 12 per cent of facilities met basic sanitation standards and that approximately 30 per cent had functional hand hygiene facilities with soap and water available. Only 6 per cent of facilities met all three basic WASH criteria at the time of measurement. These figures indicate improvement in water access relative to earlier baselines, alongside continued deficits in sanitation and hygiene that directly affect the quality of care, particularly in maternity settings.
Structural factors help explain this pattern. World Bank analyses show that access to piped water in urban areas declined from approximately 32 per cent in 1990 to below 10 per cent by 2015. Where household and community water systems are constrained, health facilities often depend on boreholes, storage tanks, or intermittent supply. These arrangements rarely guarantee water at the point of care and seldom ensure consistent hygiene between patients.
This evidence is also grounded in lived national experience. During my time as First Lady of Kwara State from 2003 to 2011, I observed how sustained political attention, institutional coordination, and community engagement could translate into tangible improvements in health and WASH-related outcomes. By 2011, Kwara had recorded steady gains in antenatal care utilisation, childhood immunisation coverage, and access to improved drinking water, in line with national and global development priorities at the time. More than nine in ten women accessed antenatal care at least once, over four in five completed the recommended number of visits, routine immunisation coverage had increased substantially from early-2000s baselines, and access to nutrition and improved drinking water had expanded to reach a clear majority of households. These experiences reinforced the importance of treating health services and basic WASH conditions as interconnected foundations of progress.
It was against this backdrop that global attention to WASH in healthcare facilities sharpened. This shift was subsequently codified within the governance of the World Health Organization itself. In May 2019, WHO Member States unanimously adopted World Health Assembly Resolution WHA72.27, entitled Water, sanitation and hygiene in health care facilities. The resolution formally recognised persistent global deficits in access to safe water, sanitation, hygiene materials, waste management, and environmental cleaning within health settings, and called on Member States to develop national roadmaps, set and monitor targets, strengthen systems and workforce capacity, and invest in sustainable WASH services as an integral component of quality care, patient safety, and infection prevention and control.
This accumulation of evidence prompted a decisive global response. In 2018, the United Nations Secretary-General issued a Call to Action on WASH in healthcare facilities, recognising water, sanitation and hygiene as foundational elements of quality care. Following this call, WHO and UNICEF strengthened global guidance, expanded monitoring frameworks, and promoted practical tools such as the Water and Sanitation for Health Facility Improvement Tool (WASH FIT) to support continuous facility-level improvement.
This reframing reflects the legacy of leaders such as the late Dr Mwelecele Ntuli Malecela, whose work consistently emphasised that maternal health, disease control, and health security cannot be separated from the environments in which care is delivered. Throughout her leadership at the World Health Organization and in earlier national roles, she advanced integrated and evidence-driven approaches that treated WASH as a core determinant of health system performance.
This systems-oriented understanding has also been advanced by Dr Maria Neira, Director of the Department of Environment, Climate Change and Health at the World Health Organization, whose work has consistently emphasised the role of water, sanitation, hygiene, and environmental determinants as foundational to disease prevention, health equity, and resilience in the context of climate change.
The global mandate was further strengthened in December 2023, when the United Nations General Assembly adopted by consensus a resolution on water, sanitation, hygiene, waste management, and electricity services in health care facilities. Led by the Philippines and Hungary, the resolution called for the systematic integration of these essential services into national health planning, financing, monitoring, and workforce development, and explicitly linked them to infection prevention and control, maternal and newborn health, antimicrobial resistance, universal health coverage, and health system resilience.
Since the 2018 Call to Action, progress has continued, though unevenly. WHO and UNICEF reporting from 2023 indicates that approximately 37 per cent of healthcare facilities in fragile and low-income contexts still lack basic water services, with sanitation and hygiene coverage remaining substantially lower than water access. Financing for WASH in healthcare facilities remains fragmented, with capital investments often exceeding funding for operations, maintenance, and sustained behaviour change.
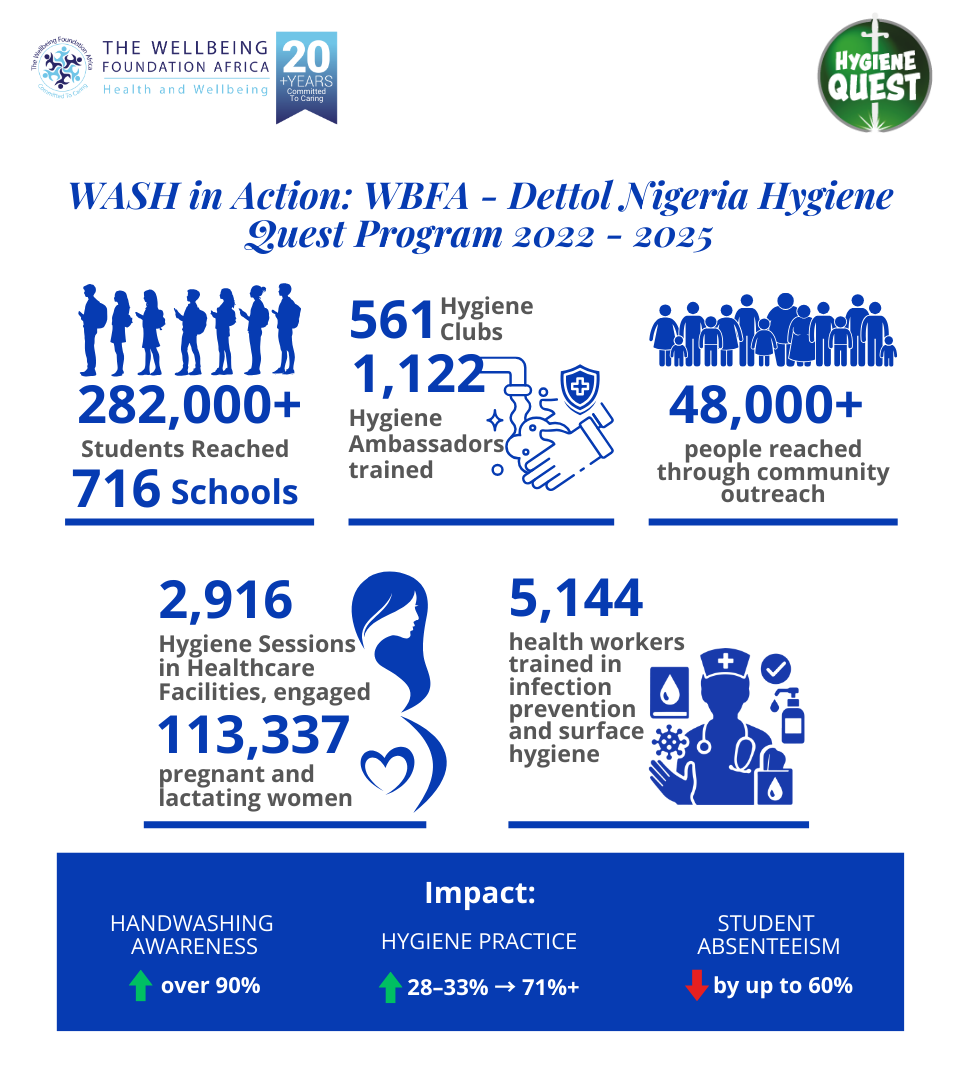
In Nigeria, applied systems work has demonstrated what targeted action can achieve. Through the Wellbeing Foundation Africa Dettol Hygiene Quest Curriculum and Programming, implemented by WBFA in partnership with Reckitt and aligned with the Federal Government’s Clean Nigeria Use the Toilet campaign and the national Hand Hygiene for All Roadmap, hygiene education has been integrated across schools, communities, and healthcare facilities.
Between 2022 and 2025, across Phase I and Phase II of implementation, WBFA programme monitoring shows that more than 282,000 students across 716 schools were reached, supported by 561 hygiene clubs and 1,122 peer ambassadors. Community outreach reached 48,110 people, while 2,916 facility-based hygiene sessions engaged 113,337 pregnant and lactating women. In parallel, 5,144 health workers received targeted infection prevention and surface hygiene training through the TEACH CLEAN curriculum.
Independent impact assessments conducted in 2024 across Lagos, Kwara and Abuja documented that hygiene practice scores among schoolchildren increased from baseline levels of 28 to 33 per cent to over 71 per cent following intervention. Awareness of correct handwashing duration increased to over 90 per cent in Lagos and close to 90 per cent in Kwara. Illness-related absenteeism among students declined from 33 per cent to 17 per cent in Lagos, from 24 per cent to 12 per cent in Kwara, and from 52 per cent to 11 per cent in Abuja. In health care facilities, hygiene counselling during antenatal and postnatal care improved reported hygiene practices among pregnant and nursing mothers, supporting safer childbirth and newborn care.
These findings point to a conclusion that is well established in global health but still unevenly applied in practice. Behaviour change and infrastructure are not alternatives. They are mutually reinforcing. Hygiene education reduces immediate risk, strengthens demand for reliable services, and supports safer care while systems are being improved. At the same time, without sustained investment in water and sanitation infrastructure, behaviour change cannot be maintained. Progress depends on advancing both together, deliberately and at scale.
Our call to action is therefore practical, coordinated, and timely. Water, sanitation and hygiene must be embedded as core quality of care indicators within national health sector plans, with dedicated and traceable budget lines that extend from national frameworks to individual facilities. Financing models must move beyond one-time construction toward multi-year support that covers operation, maintenance, consumables, and workforce capacity. Health, water and finance institutions need to work in concert, using established tools such as WASH FIT and routine facility performance data to track outcomes and sustain accountability. WASH investments in healthcare facilities should be explicitly linked to priority outcomes that matter to governments and communities alike, including reductions in maternal and neonatal mortality, infection prevention and control, antimicrobial resistance, and preparedness for future health emergencies.
This is the essence of our WASH Wednesday glocal call to action. Global evidence must inform national policy. National commitments must translate into local delivery. Moments such as WASH Wednesday provide an opportunity not for awareness alone, but for alignment, reflection, and renewed accountability across sectors and partners. The evidence is clear, the tools are available, and the cost of inaction is well documented.
This is the quiet work of health system strengthening. It rarely attracts attention, yet it determines whether care is safe, whether health workers are protected, and whether women can give birth with dignity. Clean water in a delivery room does not announce itself. Without it, the promise of quality care remains fragile. Ensuring that the foundations of care are reliable is not an abstract ambition; it is a practical obligation to mothers, newborns, and the communities that our health systems exist to serve.
H.E. Mrs Toyin Ojora Saraki is Founder & President of the Wellbeing Foundation Africa. The Wellbeing Foundation Africa works across policy, practice, programming, and partnerships to strengthen health systems and advance equitable access to quality care, with a focus on women, children, and communities.
John Oldfield is Founder & Chief Executive Officer of Accelerate Global, LLC, a strategic advisory firm supporting non-profit, corporate, and government partners to rapidly and sustainably advance water, health, climate, gender, and environmental goals.
Categories
Recent Posts
The e-health check tool is available for free at https://covid19.wbfafrica.org/ and users can access real-time updates on how to stay connected, safe, and healthy during the pandemic on Instagram and Twitter @Wellbeing_PPMD, and @WellbeingPPMD on Facebook.


